

 Subchondral bone cysts of the medial femoral condyle (commonly referred to as stifle cysts) are a common cause of hind limb lameness in Quarter Horses. According to a 2012 Equine Veterinary Journal study evaluating young cutting horses by R.D. Contino, prevalence can be as high as 10-13.6 percent.
Subchondral bone cysts of the medial femoral condyle (commonly referred to as stifle cysts) are a common cause of hind limb lameness in Quarter Horses. According to a 2012 Equine Veterinary Journal study evaluating young cutting horses by R.D. Contino, prevalence can be as high as 10-13.6 percent.
There are two proposed causes: 1) Developmental orthopedic disease or osteochondrosis, or 2) Traumatic injury to the cartilage and/or subchondral bone (bone directly beneath the cartilage). While the medial condyle of the femur is the most common location, subchondral bone cysts can occasionally occur at other locations within the stifle (lateral femoral condyle, proximal tibia, patella) as well as in other joints (pastern, elbow, fetlock, etc.).
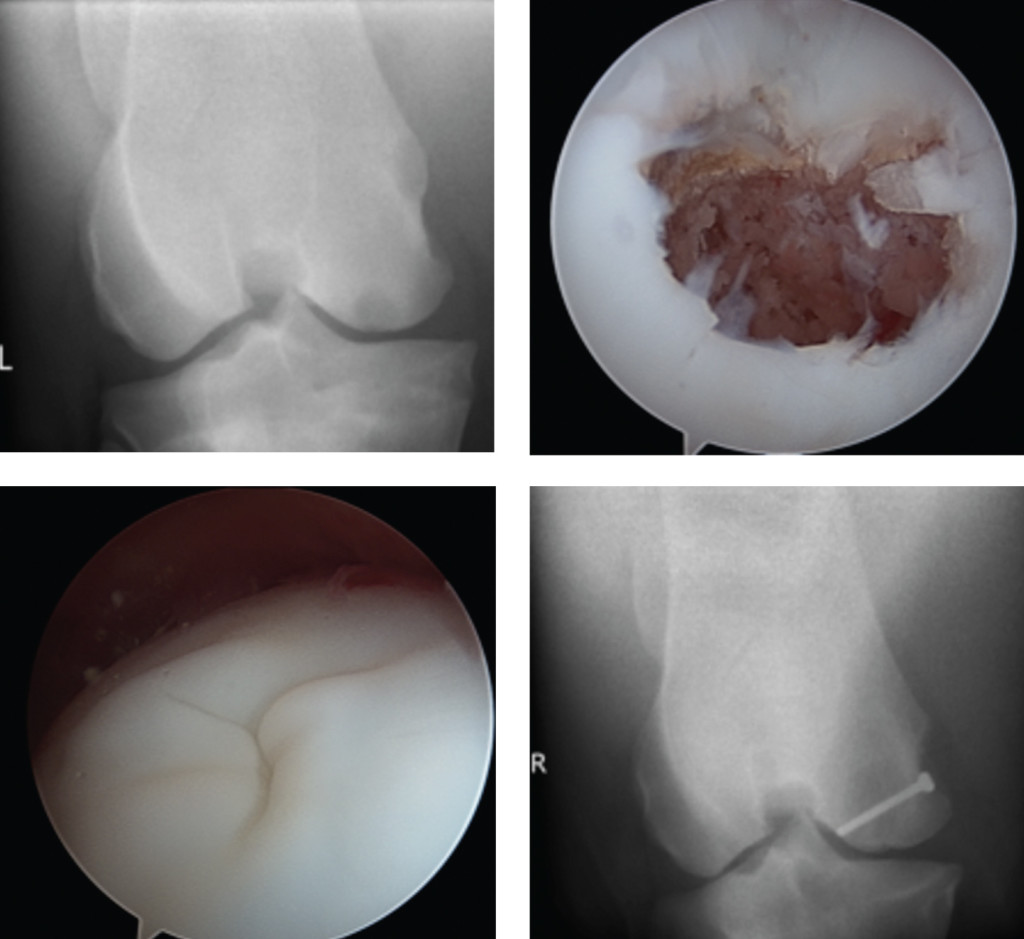
While stifle cysts are most frequently unilateral (one leg), these lesions can occur bilaterally (both hind legs). The most common presentation for a stifle cyst is a young horse, 1-3 years of age, with stiffness of the hindlimb, reluctance to flex the hindlimb and/or lameness, and often effusion/swelling of the medial femorotibial joint of the stifle. Diagnosis is made by taking radiographs, and the cyst will be evident on caudocranial and caudolateral craniomedial oblique projections. Radiographically, the cyst may be evident as a shallow concavity in the condyle, a large oval lesion a couple of centimeters in depth, or anywhere in between, and will often have a narrow neck or cloaca connecting the cyst to the joint space. Tissue within the cyst cavity has been demonstrated to contain inflammatory cytokines that may be responsible for forming the cyst and causing lameness, as well as promoting degenerative joint disease (arthritis) over time.
Treatment of stifle cysts is a topic that has been extensively researched, particularly in recent years. Conservative management (rest, anti-inflammatory medications such as phenylbutazone) has been associated with a success rate ranging from 45-64 percent, according to two 1982 studies by L.B. Jeffcott and B. Stewart. Traditionally, arthroscopic debridement of the cyst has been the treatment of choice. The philosophy behind surgical debridement is based on removal of all necrotic tissue debris and lining from the cyst cavity in order to allow the body to heal or fill in the remaining defect. Reported success rates (for return to athletic function) following surgical debridement range from 64-95 percent according to a 1995 study by N.D. Howard, 2002 AAEP convention proceedings by E.A. Sandler, and a 1988 study by N.A. White. Age is often considered a factor influencing healing of stifle cysts. According to a 2005 Equine
 Veterinary Journal Study by M.A. Smith, 64 percent of horses less than three years of age at the time of surgical debridement returned to soundness, versus only 35 percent in horses over three years of age.
Veterinary Journal Study by M.A. Smith, 64 percent of horses less than three years of age at the time of surgical debridement returned to soundness, versus only 35 percent in horses over three years of age.
After debridement, the cyst cavity is typically left open to heal; newer techniques have been evaluated to fill the cyst in an effort to enhance healing, such as cancellous bone or osteochondral (bone and cartilage) grafts, synthetic bone substitutes with bone marrow aspirate concentrate or platelet rich plasma, and growth factors with allogenic chondrocyte (donor cartilage cell) grafts with mixed results. Multiple other treatment options have been developed and evaluated as well. Injection of corticosteroid directly into the cyst lining, via arthroscopic guidance, has a reported success rate of up to 90 percent for unilateral lesions and 67 percent for bilateral lesions according to a 2008 study by T.W. Wallis.
One more recent approach to treatment of stifle cysts involves placement of a screw in lag fashion across the condyle of the femur. The theory behind this therapy is that the screw placement may promote formation of new bone within the cyst while maintaining the cartilage at the joint surface. A 2014 retrospective study by E.M. Santschi evaluating horses with stifle cysts treated with a transcondylar screw found an approximately 75 percent (15/20 horses) rate of success regarding resolution of lameness and increased density (filling in) of the cyst on radiographs.
As with traditional OCD lesions, prognosis for athleticism for horses with stifle cysts treated surgically depends largely on concurrent degenerative joint disease and/or soft tissue lesions.
Typically, age greater than three years, concurrent cartilage damage, existing osteoarthritis, and concurrent or subsequent meniscal tears are associated with a poorer prognosis and decreased likelihood of return to soundness following treatment. Early diagnosis and treatment will afford the best chance for a successful athletic career.
Megan Williams graduated from Kansas State University and went on to an internship at Ocala Equine Hospital. She completed her surgical residency at Michigan State University. Dr. Williams is a surgeon at Saginaw Valley Equine Clinic and a lameness diagnostician with GameTime Sports Medicine at major AQHA events around the country. You can email her at megan@saginawvalleyequine.com or visit her at www.saginawvalleyequine.com. You can also write to her in care of InStride Edition.
You must be logged in to post a comment Login